Human Growth Hormone: Can it help?
Category: Uncategorized
Aging discussion group meeting March 8, 2022
Daily Thesis Progress: January 2022
1/2
Printed Prolonging healthy aging: Longevity vitamins and proteins, by Bruce Ames, 2018.
1/4
Started reading Ames, 2018.
1/5
In the morning I read a bit more of Ames 2018 paper.
Today my book Blind Analysis for Design of Experiments arrived. I ordered it last month. I browsed through it a bit.
1/6
Finished Ames.
1/7
I am not getting enough journal reading in so I think I will implement a policy of 1 article per week minimum.
Finished reading Ames 2018.
Reading in Xu, 20
Printed McCann (2018).
1/10
First class of Cellular Signaling, being taught by my advisor Larry Duffy. It is a 1 hour class meeting 3 times a week.
1/11
I spent most of the morning getting ready for the 2 pm meeting of the aging discussion group, and then an hour holding the discussion. 2 new non-local members, but not so many local members showed up. Total of about 7 of us.
1/12
Class in the morning (from 9:30 to 10:30).
After class I talked about my PhD project with Dr. Duffy.
In the evening I started reading a journal article … in the future I will try to do a better job of logging these (written 2/12/22 when I was reviewing these fir posting on my blog)
1/13
Protocol-Y meeting. Very good discussion. He is starting to put together his interview series for his documentary.
He requested books we liked, so I put together a list of my books. I spent quite a bit of time after the meeting doing so. I should link it here!
When I read an aging book I usually take handwritten notes on it. But a lot of these I haven’t transcribed. I figured Tom would find them useful (and perhaps other people) so I worked on my notes from reading Spring Chicken (which I thought was the best aging book I have read).
1/14
Class in the morning.
Finished entering my notes from Spring Chicken.
Started reading Kappele’s Blind Analysis for Design of Experiments and Response Surface Methodology, chapter 1 & 2 and browsed through the appendix.
1/18
Found several interesting papers, printed 3 of them and read one
1/19
Read chapter 3 of Kappele’s Blind Analysis for Design of Experiments and Response Surface Methodology.
After a day off Monday, had class today.
In the afternoon I worked on my thesis project proposal.
1/20
Spent most of the day working on my proposal for an experiment. Did a little bit more work on my reading log, getting more information entered.
Short entry for a ton of work!
1/21
Cellular Signaling class, 9:30 to 10:30. This class actually works really well with my schedule because I drop my daughter off at 9:15 for her class in Gruening. She finishes in time to walk up to my classroom in Reichardt by the time I get out.
Comments
Introduction to Defeating Aging comments
I will confess I am not very good at using the software I use to write this blog in. Comments are a good example; I have received comments but I have not figured out how to add them into my blog. I wrote this blog to cover them, plus a few other notes.
I figured I would have a lot of time to read while on the cruise around the world so I bought a couple of books about WordPress and am now (mid-July, a bit over halfway around the world) almost finished reading them. I kept notes as I read them, you are welcome to read them. First, I read WordPress (310 pages) by George Plumley (my notes). Now I am reading WordPress for Dummies: 8 books in 1 by Lisa Sabin-Wilson [Amazon link] (I’ll add these notes after I finish). I am hoping the nuggets of wisdom I have gained from these books will help me get this blog so it looks and reads better! But it will take time; my internet access is expensive while on the cruise ($30 a day) so I don’t spend much time online (1 day a week, average). After I get home in September, I hope to be able to upgrade this website.
I am also working to build a better team to improve this blog. I have a lot of overseas contacts and several employees; I am looking to hire a nutritionist and perhaps someone who is really good with WordPress. I am also working to develop a network of doctors to assist me in clarifying medical issues related to aging. The idea is to have a team of doctors who can help apply the medicines that are coming soon to the problem of aging, assuring that health and life span is enhanced.
If you have an idea you think would make a good aging blog feel free to suggest it. I would be happy to consider any suggestions. If I get too many, I will probably put it to an online vote and whichever one gets the most I will write first!
Comments & Replies
Jose:
“Not interested in aging for myself, but for my parents. What do you recommend they do to stay healthy? They are in their 50s.”
My reply:
The first mantra of medicine is do no harm. This is difficult to impossible with someone who is suffering from an incurable disease like aging, for doing nothing results in death yet there are no real protocols that deal with it successfully. Yes, I consider aging to be a disease…one which we don’t have a cure. Yet: someday we will. The question is what can we do NOW to slow aging without causing harm? The most researched aging ‘defeater’ is calorie restriction. But you need to enter calorie restriction very carefully if you are older because it is easy to damage your metabolism, doing the harm you are striving to avoid. If you want, I can help develop a protocol for them. Nothing medical, but things your parents can try that are shown to extend healthy lifespan like additional exercise and a healthier diet. I can also use my growing network of doctors (and soon nutritionists and others) to give suggestions they can have their doctor evaluate. I would need to know what their current diet is now, and consult with a nutritionist about what changes would be good to achieve full nutrition while cutting back on calories. Personally, I have never succeeded very long in full calorie restriction. But even if they don’t succeed with calorie restriction, there are many things they can do that will gain some of the benefits of eating less…without quite so much hardship. Let me say again: anyone over 40 should not restrict calorie intake without being very careful about how they do it because you can permanently damage your metabolism by doing so.
Calorie restriction is very difficult. It has some drawbacks like not being able to stay warm (already a problem for the elderly). Daily exercise is a little easier. I have a good friend who is over 80 and in good health; he has conquered multiple sclerosis and keeps fit with a vigorous 20 minute walk every day. Anyone who exercises 45 minutes a day can extend lifespan somewhat. Even more important is the health they gain: exercising will fight off sarcopenia (muscle wasting). I have seen many people who exercise regularly stay healthy up to within a year of death, avoiding up to 2 decades of frailty and morbidity. If your parents are interested in exercise, I recommend reading book $*$[italic, Amazon link] Younger Next Year by Chris Crowley & Henry Lodge ($*$*link my notes). This will help them understand the importance of exercise and help design an exercise regimen. In brief they suggest 45 minutes of exercise 6 days a week. 2 days a week with weights, which is necessary to slow sarcopenia, or the muscle wasting you see in so many of the very old, and 4 days of aerobics to keep your heart and lungs in good shape. If they are not used to exercising, I suggest seeking professional help to get started. It also helps a great deal to try to make it fun…if it isn’t fun exercise becomes a chore which I at least tend to skip far more often than I should.
Staying socially engaged is also really important. If they do not have a lot of friends or close family, I suggest they look for social activities they like. Perhaps choose a biking club or go dancing with friends and get exercise along with socializing? Being socially active (friends, family, or anyone you can become good friends with) is one of the keys to maintaining good brain health. [$*$*italic]You can help here by spending as much time with them as possible, a minimum of several hours a week will help keep them mentally engaged by thinking about you and your activities. Face to face, if possible. By phone or video chat if not.
A form of socializing is staying employed. Many of those who stay employed enjoy a longer and better life. Those who retire and sit on the couch watching TV usually shorten their lifespan considerably—and their health span even more. If you don’t want or need a paycheck or the rigors of work perhaps find a worthy cause to volunteer for? Keeping mentally engaged provides all kinds of benefits, from better fitness to improved cognitive function!
Brain health is also determined by the foods you eat. I track all the foods I eat and use a spreadsheet[$*$*link] to calculate my nutrition for nearly 50 nutrients. The most important 4 nutrients for me are fiber, potassium, magnesium, calcium and sodium and zinc. The first 4 I sometimes struggle to get enough of and the next one I tend to eat too much of! Zinc I seem to be perpetually low on so when I feel like I might catch a cold, I take a zinc pill so that usually keeps me within the RDA (recommended daily allowance). Brain health is also controlled by the B vitamins and quite a few other nutritionally related things. I suggest you read my previous blog about defeating dementia[$*$*link] for more information.
Keeping blood pressure low is something everyone should pay attention to. Your parents should have it checked and try to achieve the current recommendations, which are a blood pressure less than 120/80. If theirs is higher than that, they should take steps to lower it. Losing weight, exercise and diet are all ways to help controlling blood pressure. Mine is too high and this summer I am working very hard to get it down; if I fail, I will have to take pills to control it because it is over 120/80. Anyone with blood pressure over 140/90 should talk to a doctor right away to discuss options to get it down to safer levels. I use a home blood pressure cuff; these are easy to use and fairly accurate if you get an arm cuff. I haven’t gotten good results with the ones that go on your wrist because the readings vary pretty widely for me. Because I am so concerned about my blood pressure, I take it every morning right after I get up. I recently wrote a blog about salt (which is where the majority of your sodium comes from) and high blood pressure[$*$*link]. Only about 10% of people are sensitive to salt but for anyone who has high blood pressure it is worth investigating. When I was talking to Dr. Alan Green, he mentioned that there are some people who think low salt intake will also increase your lifespan. I plan to investigate this further.
These are the most important things proven to help your parents remain healthy into old age. There are a number of drugs that look good right now, but have not been proven as treatments for aging. Drugs like senolytics (which kill bad cells), rapamycin (which partially resets your aging cells) and metformin (which improves metabolism) have all been shown to extend lifespan in mice and other animals. Clinical trials are underway with some of these, results coming.
There are a number of groups around the world, such as the Okinawans (Japanese who live on the Okinawa island), who live to extreme old age. This is usually determined by 3 factors in their lives: their diet, their social life and the exercise they get. Adopting a lifestyle similar to them will enhance your parent’s chances of a healthy old age. The coming drugs will enhance this further, and perhaps extend their life span significantly.
To help them more than general suggestions I would need more details. If they would care to contact me please tell them to feel free to do so. If nothing else I hope I have suggested a few things that will help them. A successful outcome is dependent on many factors so it is difficult for me to suggest anything more without a more personal interview.
[$*$*horizontal line]
Akio
re: Medical testing, PCS9 inhibitors & aging conference–an email to a friend
“Just time today for a quick look. Will come back for more later. Interesting so far.”
My reply:
I hope you manage to stop by again. If you send me a note[$*$*link] I will add you to my mailing list, which is small but growing. Please note if you want an email with every blog, or just a quarterly review (every 3 months). The email will provide a synopsis of the blog and a link so if you are interested you can read all of it. Also let me know if you want a free copy of the book I will be writing about aging; hurry though, not many are offered for free. At some point I may offer this blog as a printed newsletter, but I have a bit to go before I am organized to do that–and I may have to charge to cover my postage.
[$*$*horizontal line]
Jenny:
re: Dementia blog
“My husband seems to be losing his mind. He can’t drive because he gets lost before he gets to the freeway. We are having to sell the business because his memory is so bad. Our doctor says it is a ‘fact of life’ and my husband ‘has had it’. What do you suggest? We need Help!”
My reply:
Dr. Bredesen mentions a case very similar to your husband’s, where the lady he discussed could not remember how to find her way and was leaving work for similar reasons. Your doctor does not sound very promising, but he may just be frustrated with the lack of options. I suggest you buy a copy of [$*$*italic]The End of Alzheimer’s [$*$*link to my blog] and read it. If you think it would help take it to your doctor…if he doesn’t think Dr. Bredesen’s ideas will work perhaps you can get a second opinion.
I do not see it as my position to give medical advice, nor would it be legal for me to do so; I am not a doctor. My aim with this blog is to provide information so people can understand the options that are available, like Dr. Bredesen’s protocol for dementia, or testing if you are salt sensitive and can use salt as a means to controlling high blood pressure.
I also want to showcase the coming treatments that slow old age, so people can understand that there is a real chance of living a lot longer than expected, and in much better health. In a few decades much of what I write about will be mainstream. If you can take the steps now to preserve your health (like exercising more and eating right) you will have a better chance at being in good health when more advanced treatments like senolytics[$*$*link] or rapamycin[$*$*link] become available.
Good luck!
[$*$*horizontal line]
Jerry:
“I don’t believe this stuff! You get old. You get dementia. That is a fact of life and you can’t avoid it. Why should I take your word for it?”
re: Demetia blog
My reply:
You shouldn’t take my word for it! When you read something online like my article about Dr. Bredesen’s protocol for reversing dementia you need to research it yourself–or take it to your doctor and have him do so. Nothing you find online should be accepted as the whole truth; most of it is just people’s opinions. I find it hard to believe that some people believe so much in what they read online that they will go out and kill someone–I heard of a case in central America where a guy was so demonized on social media that a group of villagers attacked and killed him all because someone started a rumor about him being arrested. Either it is true, in which case the internet contributed to the guy’s death…or it isn’t true, in which case it highlights you can’t believe what you read online! So always look for multiple opinions from someone who understands what they are talking about, especially when it is as important as your health!
Do I know what I am talking about? When it comes to aging, I have been studying aging since the late 1970’s. I obtained a BS in Biology and am now working on a PhD. Since 2000 I have accelerated my aging studies, and regularly read all the journals in the field as well as attend an average of 1 conference a year. So, I am confident I understand the fundamentals of science’s current position on aging. Do I know enough to give medical advice? No. But I do know enough to suggest where you might find the kind of medical advice you need and to point out the things that have worked for extending healthy lifespan in mice and monkeys may also work in people. I also have many contacts with doctors who might be able to advise you about specific problems like high blood pressure.
So, take my ideas and explore the avenues that interest you. But do your due diligence before taking action! Some things like eating a daily handful of sunflower seeds if your vitamin E consumption is low need no further explanation; some things like having vitamin B injections for low vitamin B levels should be done under competent care to you assure you get just what you need; not too much and not too little.
[$*$*horizontal line]
Albern
re: Dementia blog
“So you say lot of things to test, but did not do all. Do you think this is enough?”
My reply:
No. We do not know enough to completely reverse or stop dementia. But the testing suggested is based on hard science, and each factor has been shown to be one of the causative factors in dementia. We know a little, and that little is enough to have a positive impact on those getting dementia. While the hype says ‘cure’ that remains uncertain because for me a cure means ‘gone and will not come back’, and only time will tell if protocol developed by Dr. Bredesen will provide a long-term solution. More solutions are likely as the network approach to medicine (that is many medical issues are caused by more than one issue and so for a complete cure for anything requires fixing multiple issues) expands.
[$*$*horizontal line]
Kraig
“Read through the site. Thanks, Ray. Glad you are posting this stuff. Sorry to hear of the passing of your godfather and uncle. As you noted, we are always poorer for the loss of our elders as well as suffering the personal loss. My condolences, dear friend. I will return to this site from time to time to keep up on the latest. You can use my name freely in your postings, if you like. It doesn’t matter to me, either way. Kraig. P.S.: Count me in on the book of course! :)”
My reply:
Thanks Kraig. Encouragement is really helpful; sometimes it is hard to turn out quality product when you get little feedback! Yes, it is so sad to lose people you are close to; as we get older our friends die one by one. I imagine this is really bad for your mental health, not to mention really sad. My godfather did not have any friends left from his generation; my Dad was his best friend and died 15 years before he did. Death is the enemy: I hope science conquers it and my son sees the end of aging and death before he gets old in 40-50 years. I even feel that with the right approach people our age may have a small chance of living long enough to see real progress toward defeating aging.
I have added you to the book list 🙂 For those of you reading this: if you want a free book, I will send you one–if you click$*$* soon enough!
The Longevity Seekers by Ted Anton: My notes.
I bought The Longevity Seekers in 2016, at the same time I bought a large number of other aging books. So it wound up on a shelf and by the time I left for a cruise around the world 3 years later I still hadn’t read it. So I brought it with me.
I started reading it on June 1st (2019) and finished reading it on June 6. It turned out it was a really good book, well written and entertaining, as well as having a lot of information about the pace at which aging science exploded between 2002 and 2013 when the book was published. Now I wish I had read it long before…
These are my notes on the book, listed here partly for my own use but also so my readers can have an idea of the book and perhaps encourage them to buy it.
These are my notes from reading the book:
Pg 4: Some of the theories of aging.
Pg 4: Hayflick limit (this is the number of times a cell will replicate).
Pg 5: Clive McCay in 1934 published “Prolonging the Lifespan” in which he observed calorie restriction extended the lifespan of rats and mice by 40%.
Pg 5: Walford’s book “Maximum Lifespan” published in 1983 which is what drew me firmly into the scientific field of aging. Before this book I had been keen on the subject, but this was the first hint that lifespan was flexible.
Pg 6: Disposable soma theory of aging. [$*$*link]
Pg 8: Some cells are programmed to die.
Pg 8: Just a few similar genes determine development (body plan) in many different species.
Pg 9: Paramecium rejuvenate after sex and grow old if they don’t reproduce sexually.
Pg 11: “Aging was an intractable scientific problem.”
Pg 14-22: A chapter about Cynthia Kenyon, one of the great aging scientists.
Pg 18: Stanley Prusiner discovered prions and Elizabeth Blackburn discovered telomeres.
Pg 18: The HOX genes.
Pg 20: daf-2 mutant genes doubles lifespan in C. elegans (a tiny worm).
Pg 21: daf-16 is needed for lifespan extension with daf-2.
Pg 24: Michael Rose tricked flies into extending lifespan by only allowing late breeding.
Pg 25: “Ageless Quest” book (autobiography) by Leonard Guarente.
Pg 27: Yeast UTH gene extended lifespan in yeast but also caused infertility.
Pg 30: NAD is made from Vitamin B3 (niacin).
Pg 32: Early aging gene discoveries stimulated many new researchers.
Pg 36-7: The worm daf-2 is insulin (basically).
Pg 40: Pope Innocent VII tried to revive himself with a blood transfusion from a young man (1942).
Pg 47: Ames Dwarf mice have a mutation in PROP-1 (pituitary factor-1) and live 50% longer because of it.
Pg 48: Long life linked to smaller size, but to a lesser extent in humans.
Pg 45: SAGE KE = Science of Aging Knowledge Environment (from internet: Active from October 2001 to June 2006)
Pg 49: Adrzej Bartke made a flowchart of aging theories
Pg 67: Worms modified to live 6 times longer, and 2 of them lived 10 times longer (same as a person living to 780 years old!!)
Pg 69: Metformin increased mouse longevity by 38%
Pg 69: AMPK = cell fuel gage
Pg 71: Book: The Structure of Scientific Revolutions by Thomas Kuhn
Pg 73: Molecular biology of aging made many theories of aging merge toward antagonistic pleiotropy
Pg 74: Adrzej Bartke showed that the insulin pathway worked separately from calorie restriction and when both were applied it doubled mouse lifespan.
Pg 74: Computational biology of aging is a new field in (2005?)
Pg 75: Calorie restriction started in middle life increased lifespan by increasing APM-kinase which increased FOXO.
Pg 75: Brunet lab has public and foundation funding.
Pg 76: Gene chips showed only a few genes change their transcription rate in aging.
Pg 77: Can measure aging by measuring lipofuscin levels
Pg 77: “Aging is not programmed” says Steve Austad
Pg 79: Easter Island statues “look out to sea” <–wrong
Pg 80: 20 month old mice given rapamycin lived 20% longer. This is like a 60 year old human getting 20 years of healthy life instead of 10.
Pg 81: Valter inhibited mTOR and extended yeast lifespan by 10 times!
Pg 81: Rapamycin cost (2005?) $1,000 a week.
Pg 81: The Biology of Aging, a book by R. Arking (Observations and Principals)
Pg 82: Cells treated with resveratrol increased in number and health of mitochondria.
Pg 83: Resveratrol decreases the impact of a high fat diet and increases health of mitochondria.
Pg 87: Sequoia live to 1,000 years old.
Pg 88: Bowhead whales live to 200 years old.
Pg 91: Effect of an individual’s genes shaped by diet, environment experience and chance.
Pg 91: Grandmother theory (last paragraph).
Pg 91: Kinship dynamics is a new field about grandmother effect.
Pg 92: Seabirds maintain telomere length their whole life.
Pg 93: Naked mole rat has stress-protected version of Nrf2, “which preserves to power of proteins to fold properly”.
Pg 93: Many late-life illnesses are disease of protein folding.
Pg 93: Chaperone proteins unfold and refold bad proteins.
Pg 94: Dutch in WWII famine (pg 95) led to epigenetic changes if first 3 months of gestation were in starvation.
Pg 95: FOXOa gene found in Ashkenazi Jews and others.
Pg 97: GlaxoSmithKline restructured to be units no bigger than 100 people.
Pg 98-9: Aging is a network.
Pg 103: Rando says “[aging]…decline in structure and function. The cause is a network of influences and effects with…nonlinearity and feedback.”
Pg 105: Brunet studied overlapping networks of FOXO3/calorie restriction/AMP-kinase.
Pg 105: Rapamycin extends lifespan in older mice by 30%.
Pg 106: FOXO gene triggered in worm body sets it’s embryo clock to 0.
Pg 106: Genes influence health aging by slowing it, molding it, etc.
Pg 106-7: Four molecular pathways make overlapping networks modulate longevity.
Pg 109: Derek Lowe runs a blog.
Pg 107-110: Resveratrol does not appear to affect lifespan.
Pg 111: Evolutionary distance between (human:fly) is less than (fly:work)!
Pg 115: “Proper protein shape is a key to late-life health.”
Pg 115: Misfolded proteins clump and clog signaling pathways and play a roll in aging diseases from cancer to Alzheimers and most significantly heart disease.
Pg 117: “Aging is a network of feedback loops in humans.” says Erik Kapernick.
Pg 117: 247 known or suspected longevity genes.
Pg 119: Metformin tested in 1,100 clinical trials!
Pg 122: Cancer is rare in young people because they use same cytokines as those used by the naked mole rat to attack damaged cells.
Pg 125: Epigenetics causes “gene scars” in aging lab animals.
Pg 125: Stem cells of cancer patients age faster than normal.
Pg 125: Epigenetics ==> “cell response to DNA damage is probably more important to aging than the damage” says David Sinclair.
Pg 131: FOXO gene extends lifespan when activated and can be activated by diet.
Pg 132: FOXO3a prevents bone loss.
Pg 132: Centenarians have more and larger HDL, controlled by the CETP gene.
Pg 132: Mitochondria secrete peptides that decrease with age that have anti-diabetic, anti-Alzheimers and anti-atherosclerotic properties.
Pg 133: A single gene does not create a single protein, but many.
Pg 133: Book: “Genes and What to Make of Them” by Barnes & Dupre.
Pg 134: Encyclopedia of DNA elements (ENCODE) suggested most DNA diseases are caused by switching errors.
Pg 137: “Aging programmed…proteins fall apart…[stop] reproduction.”
Pg 137: To live longer need to hit 2+ longevity programs.
Pg 142: List of non-profits about aging or that serve old people.
Pg 142: From 1990 to 2008 lifespan decrease about 3 years for males and 5 years for females.
Pg 144: By 2050 human lifespan will increase as much as 30 years.
Pg 148: Olshansky’s PhD thesis = new ways to calculate life expectancy that is still in use by some insurance companies.
Pg 149: Olshansky book: “The Quest for Immortality”.
Pg 150: UK fertility rate fell from 5 per woman to 2 took 150 years; South Korea it took 20 years (1965 to 1985).
Pg 151: Vitamin D in milk.
Pg 152: Memory is improved by motivation to improve.
Pg 154: Volunteerism is worth $272 billion in the US.
Pg 155: Fasting during chemotherapy increases resistance to radiation.
Pg 155: Mitochondria mutate as we age.
Pg 156: Science is never perfect.
Pg 158: 4 major signaling pathways control aging rate.
Pg 159: Epigenetics can be inherited through 4 generations.
Pg 164: By 2014 there were 1,400 clinical trials for rapamycin, 1,100 for metformin, 58 for resveratrol, 11 for mitiglinide, a blood-glucose lowering drug.
Pg 164: Sirolimus is the drug name for rapamycin.
Pg 165: Private money poured into aging research.
Pg 166: 1.5-2 billion invested in aging in “the last decade” (2002-2012?)
Pg 167: Aging is still an immature sciences, in the adolescent phase of rapid growth.
Pg 171-5: Where people mentioned in the book currently are (as of publishing in 2013).
Pg 179-80: Longevity gene timeline.
Pg 183: McCay’s reference (1934).
Pg 187: Reference to “A cause of Yeast Aging” in Cell 1997.
Pg 211: Reference to clinicaltrials.gov (resveratrol)
Salt Sensitive…or not?
Slowing aging is partly about reducing the odds of sudden death. Stroke and heart attack are two of the leading causes of sudden death in the world, so I am pretty concerned about them. I figure any way I can reduce the chances of stroke or heart attack will improve my chances for living longer. High blood pressure greatly increases my chances of having a stroke or heat attack.
My blood pressure has been higher than it should be for several years now. My Thai and Sri Lankan doctors are not concerned because it is not in the hypertension range, and they tell me that my blood pressure is within the normal range for someone my age (134/84). But that is now considered high by doctors in the US, who have recently upgraded their recommended maximum blood pressure to 120/80 (if you are over this you are considered hypertensive; before you weren’t considered hypertensive unless your BP was 140/90). By this new definition I am definitely hypertensive.
I have tried a lot of things to keep my blood pressure low over the years without much success. I have tried losing weight; exercise; meditation; mostly following the Dietary Approaches to Stop Hypertension (DASH) diet; reducing stress; going for long walks; . The approaches that worked the best for me were losing weight and exercise. The DASH diet seemed to help a bit but not a lot. Other things did not have much, if any, impact. One thing I have not tried until now was to get my salt intake down under an average of 1,500 mg a day. While I have occasionally gotten my daily consumption below that, only very seldom have I managed to get my weekly average below 1,500 mg of sodium a day.
Sodium is a critical nutrient, and in prehistoric times it was hard for people to get enough of it. Most animals still have trouble, which is why salt licks are so popular with a lot of herbivores (carnivores probably get enough salt from the meat they eat). The theory goes that it tastes good to encourage us to find salty foods to assure we get enough in our diet. Unfortunately it is also a good preservative since salt inhibits bacteria, so most processed foods like canned food or lunch meats have a lot of salt in them.
Salt is made of up of a sodium atom (Na, which weights 33 grams per mole) and a chloride atom (which weighs 35 grams per mole). So a mole of salt is 58 grams, about 40% sodium by weight. When you put 100 mg (100 milligrams is about 1/33 of an ounce, or a pinch) of salt on your eggs, you will get almost 40 mg of sodium and around 60 mg of chlorine (which isn’t important to us here as it is usually easily excreted). This isn’t much, but when you look at how much sodium is in a cup of mashed potatoes you are eating about a gram of salt, or 600 mg of sodium. That is almost 25% of your recommended daily allowance (RDA) for sodium, or 40% of the DASH diet sodium goal! This makes it difficult to eat very much mashed potatoes without risking exceeding your RDA.
Nutrient levels in a person is based on flows. Inflows from food, air and water. Outflows through urine, feces, sweat air and surface loss (skin, hair and nails). For sodium the most significant loss is through urine and sweat. To have the right amount of sodium in your body your consumption needs to balance excretion. Your primary source for sodium is salt in your diet. You lose the most salt through your urine or your sweat, with insignificant amounts lost from breathing (the water vapor that leaves in your breath contains a small amount of salt) and in your feces. Loss through sweating is highly variable and depends on how much water you sweat. Because everyone has a different skin area, has different temperatures at which they sweat at and probably a lot of other factors it can become very difficult to calculate. But if you weigh yourself before and after a hard sweaty exercise you can get an idea. Your sweat has about 500 mg of sodium per pound of sweat. I estimate when I am sweating hard I loose a bit over 2 pounds of sweat per hour (this is how much weight I loose in an hour of hard exercise). So when I am sweating hard I estimate I lose about 1200 mg of sodium salt an hour.
The DASH (Dietary Approaches to Stop Hypertension) diet recommends consuming less than 1,500 mg of sodium a day. Since salt is made up of sodium and chloride, 1,000 mg of salt contains 396 mg of sodium. To get below 1,500 mg of sodium I have to eat less than 3,800 mg (or less than 4 g) of salt a day. This seems like a ton of salt to me. But when you start eating processed food this isn’t very much. A 3 ounce serving of Canadian bacon, for instance has 3 grams of salt! Since I log all my food I know my sodium consumption is a lot higher than the diet recommends, so I have always tried to keep my diet low in salt by not putting salt on any food except. Unfortunately, this is not enough; my normal foods I eat already has too much sodium. Bread has a lot of salt, as do meats and most processed foods. Not just a little either; just 1 slice of bread has 10% of your DASH diet sodium for the day, and 3 ounces of smoked salmon has nearly half, a can of chicken soup 2/3!
What happens if you aren’t getting enough? Sodium is needed by your body for proper neuron function, ion balance in your cells and many other things. If you are low on sodium one symptom I came across as a sign you are low on sodium was muscle cramping…but that is caused by many other things too. With our modern diet the odds of being low on salt are tiny. Sodium is key to neuron signaling, so another symptom is nerve related issues.
Too much sodium can lead to a number of problems. It can cause high blood pressure, it is hard on your kidneys and can cause your hands and/or feet to swell. My big issue is high blood pressure so while I am on this cruise around the world I thought I would try to reduce my salt consumption to see if my blood pressure responded. My kidney tests have always been good, and I drink plenty of water, so I think if I have an issue with sodium it is my blood pressure.
Even though I only put salt on eggs (and seldom have eggs), my diet seems to perpetually have more salt than recommended. More recently with all the good food on the cruise I am on right now it has been occasionally getting up over 4,000 mg. My daily average over the last 3 years has been around 3,400–see graph–or almost 1,000 mg more than US 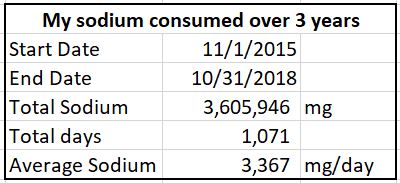 FDA’s recommendation of 2,300 mg [1]. I have been thinking about cutting out salt to get it below the DASH limit for some time so when someone blogged about not being sensitive to salt so I wrote and asked how they knew. They replied that they just reduced their salt for a week, then increased their salt for a week all the while recording their blood pressure. If there was a change then they were sensitive, if there were no change then they weren’t. My sodium intake is definitely on the high side. The question is whether it impacts my health.
FDA’s recommendation of 2,300 mg [1]. I have been thinking about cutting out salt to get it below the DASH limit for some time so when someone blogged about not being sensitive to salt so I wrote and asked how they knew. They replied that they just reduced their salt for a week, then increased their salt for a week all the while recording their blood pressure. If there was a change then they were sensitive, if there were no change then they weren’t. My sodium intake is definitely on the high side. The question is whether it impacts my health.
A couple of weeks ago I decided to see if I were salt sensitive. It was nearing the end of May and I was up for my monthly 3 day fast where I don’t eat anything for 72 hours, so I figured that would be a good time to start (perhaps…when you lose fat you may gain some salt from the fat, though I am hoping the normal salt loss was greater). I also decided to increased my water consumption to help flush salt out of my system.
After my fast I was more careful about what I ate, keeping things that have salt to a minimum and logging all my foods (which I do anyhow) to monitor salt intake. Thus by 7 days into my trial my average daily sodium intake had fallen below the DASH recommendation of 1,500 mg a day. This is the log of my salt consumption, blood pressure and other notes I recorded:
2019
5/30 0 mg Na (fasting). Blood pressure 134/84.
Drank 1,230 g of water today. I set up a spreadsheet to track my weekly average salt consumption. To set it up and give me a starting point I went back a week, so my starting level was an average of 3,350 mg/day for the week before I started my trial. I am not sure what the half-life of salt is in a person, but that is really the number I should be using, but this is probably a really good approximation and I use it for all my nutrients.
5/31 0 mg Na (fasting). Blood pressure 134/88.
I drank 585 g of water today. My blood pressure is usually up a bit when I fast, so this was not a surprise.
6/1 1,361 mg Na. Blood pressure 138/91.
I drank 1,294 g of water today. After 3 days (72 hours since my last dinner Wednesday evening) of fasting I had dinner. I was not very careful of what I ate so in this meal alone I had 1,361 mg. The thing I ate with the most salt at 310 mg of sodium for half a cup was mashed potatoes, though the thing with the most per gram consumed was the salad dressing. The things with the least salt were the raw fruits and vegetables.
6/2 1,140 mg Na. Blood pressure 132/81.
I was really careful to avoid foods with salt today, and as a result actually ate less all day than I’d eaten the evening before. The thing with the most salt were the pancakes, with almost 400 mg of sodium for an 8″ pancake. Again the foods with the least salt was the raw fruits and vegetables. Pears actually had 0 salt.
6/3 2,508 mg Na. Blood pressure 127/86.
I missed my goal today, eating too much salt, mostly through eating too much food (2487 kcal). The worst things were the oatmeal provided 330 mg; 2 T ranch salad dressing had 200; the bread that I ate (2 slices plus a dinner roll) added up to 490. The best were, again, fruits and vegetables with 0 mg in the orange I ate. However even though I fell off my goal I was off the ship (I am on a cruise ship going around the world as I do this test) and I spent 2.5 hours just pouring off sweat because I was walking around in 97 F (36 C) degree heat and high humidity, so I hope that I managed too offset some of my high salt consumption. However this is the first day my 7 day average fell below 1,500 mg (my goal), at 1,377 mg (see graph).
6/4 2,073 mg Na. Blood pressure 123/84.
Today I tried to be careful, but did not manage to keep it down where it should be. In spite of this my average salt consumption stayed below my goal of 1,500 mg (mostly from fasting for 3 days).
6/5 2,457 mg Na. Blood pressure 134/85.
Today I really failed to keep my consumption of salt down, but the ship was in Dubai today, and again I spent a certain amount of time too hot and sweating, though probably not enough to offset my higher salt consumption. Even so I managed to keep it under the RDA, if not below the DASH diet recommendations.
6/6 0 mg Na. Blood pressure 137/88.
Thursdays are a fast day for me, so my salt consumption was 0.
6/7 1,426 mg Na. Blood pressure 133/86.
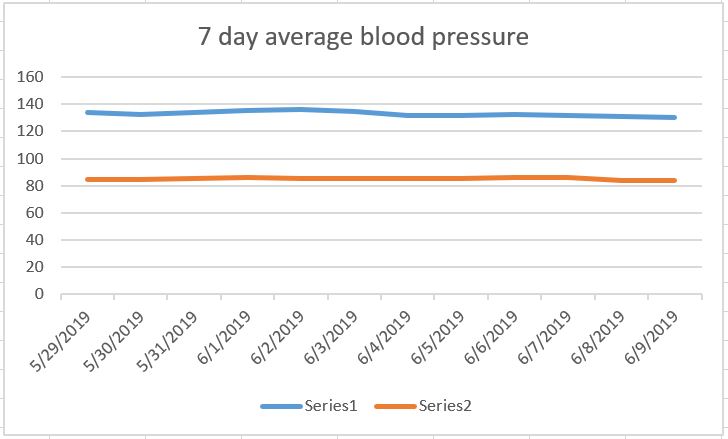
At an initial evaluation, 3 days after my average salt consumption fell below 1,500 I see that my 7 day average systolic blood pressure is down about 2 points, from 134 to 132. However, my average diastolic is up about 1.5 points! From about 84.5 to 86. So, I decided to extend the test out for a few more days to evaluate if this was a real reaction or just normal variation, since my average intake has only been below the DASH diet recommendations for 3 days; a week would be better. Then comes the other half of the test, where I try to eat a lot of salt.
6/8 658 mg Na. Blood pressure variable, probably around 129/79.
Because I am traveling and I wanted to keep as much of my weight allowance as possible for books (I brought a lot of books about aging with me for this cruise) so I brought my wrist blood pressure cuff instead of my arm one. Unfortunately this sometimes causes problems like today when I just could not manage to get a good reading:
Systolic Diastolic Pulse
119 66 60
131 83 54
138 77 50
119 82 59
I finally sort of fudged the numbers around a bit and settled on a blood pressure of 129/79. No idea if this is correct or not but it is the best I can do. I am hoping the 9th I will get a better reading so I can know if this drop in pressure is real or not. I had planned to stop the trial at this point, but because there is a sudden sharp drop (assuming these numbers are correct) I shall continue this trial until at least Sunday.
My 7 day average blood pressure before today was 132/86. So 129 is a drop of 3 points on the systolic and 79 is a drop of 7 points on the diastolic. If the numbers continue to slide, or even stay this low, I will consider salt a successful ‘biohack’ for me.
Because this is such a sharp drop I decided to keep my salt consumption down for a while longer to see if I got a further response. Because I measure my blood pressure in the morning (before eating) the low salt today has no bearing on today’s blood pressure reading.

6/9 1,369 mg Na. Blood pressure was variable again, estimated at 127/80.
My 3 day fast is starting to fall off the weekly averages, and because of that my average salt consumption for the week ending yesterday was creeping up. By reducing my consumption of salt yesterday I managed to push the weekly average down below 1,500 to 1,466.
Because sweating is a means to losing sodium I decided to start logging how long I spend sweating each day. While this is usually based on exercise it can also result from being too hot. We spent 2.5 hours walking around in high heat (95 F, 35 C) and humidity while were in Muscat, Oman on June 3. So I logged 150 minutes of sweating hard that day. 2 days later in Dubai it was also really hot, but not as humid and we spent the majority of the 6 hours we were ashore inside air conditioned buildings so I only count 20 minutes of sweating. The other days I referred to my exercise log to determine how much time I spent sweating.
I am trying to post one blog a week, but this experiment has a long way to go, so I am going to publish it in 2 parts. Part 2 will come along in about a month, after I have time to finish this experiment! Since my blood pressure seems to be responding to lower salt I will probably continue a low salt diet for quite a bit longer (2 weeks?) to assure it is not a measuring artifact. When I feel my blood pressure has either leveled off at a lower value or it goes back to the original and stays there for awhile I will do the 2nd half of the experiment: increasing my salt intake. See if my blood pressure goes up in response.
References & more reading
Sodium consumption
[1] US Food & Drug Association salt recommendations
https://www.fda.gov/consumers/consumer-updates/lowering-salt-your-diet
[2] CDC
Click to access sodium_dietary_guidelines.pdf
Dash diet
[3] Great explanation from the Mayo Clinic about the DASH diet
https://www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/in-depth/dash-diet/art-20048456
[4] Dash Diet [this is mostly just an ad to buy the book]
http://dashdiet.org/
[5] DASH eating plan from the U.S. National Institute of Health
https://www.nhlbi.nih.gov/health-topics/dash-eating-plan
[6] Ideas for starting the DASH diet from WebMD
https://www.webmd.com/hypertension-high-blood-pressure/guide/dash-diet#1
[7] US news article about the DASH diet
https://www.webmd.com/hypertension-high-blood-pressure/guide/dash-diet#1
Salt regulation
[8] National Institure of Health
https://www.nih.gov/news-events/nih-research-matters/how-body-regulates-salt-levels
[9] Journal article about how high salt affects sodium output of the kidneys
https://www.ncbi.nlm.nih.gov/pubmed/28414302
[10] Sodium loss in sweat
https://www.active.com/nutrition/articles/salt-and-athletes-shake-it-or-leave-it
[11] Sodium lack from Mayo Clinic
https://www.mayoclinic.org/diseases-conditions/hyponatremia/symptoms-causes/syc-20373711
[12] Sweat produced per hour
https://www.active.com/triathlon/articles/cracking-the-code-on-sweat-rates
[13] Scientific article about sweating
https://www.ncbi.nlm.nih.gov/books/NBK236237/
